Acute ischemic stroke.
LKW vs symptom-onset framing, imaging gates, 2026 BP targets, extended-window IVT, EVT for LVO with parallel IVT, and the posterior-circulation pitfalls that get missed. Tenecteplase 0.25 mg/kg is now Class 1.
Reviewed June 2026 · verify against current guidelines
Diagnosis & Workup
Recognize. Confirm. Stage.
Initial assessment
- Time: last known well (LKW), not symptom recognition. Wake-up = last seen normal.
- NIHSS: 0 mild to 42 max. ≥6 typically suggests LVO.
- Workup: glucose, BP, ECG, focused exam.
Imaging
| Non-contrast CT | Rule out hemorrhage. Only image needed before IV thrombolysis (IVT) in the 4.5 h window. |
|---|---|
| CTA head/neck | Identify large vessel occlusion (LVO: ICA, M1, basilar). Triage to endovascular thrombectomy (EVT). |
| CT perfusion / MR DWI-FLAIR | Extended windows (4.5-24 h). |
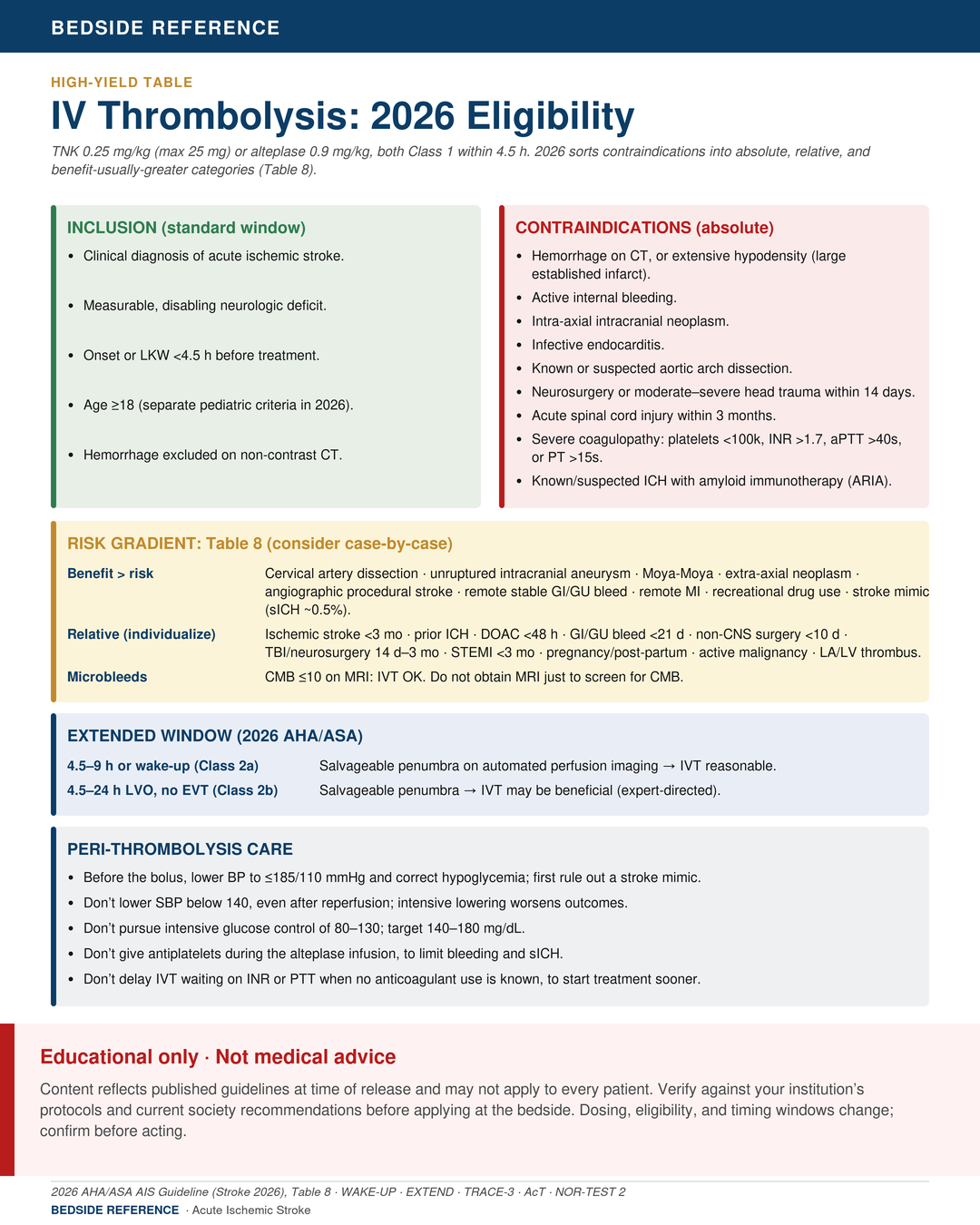
BP targets (2026)
| No IVT or EVT | Permissive HTN. BP <220/120: no Rx in first 48-72 h. |
|---|---|
| Pre-IVT or EVT | SBP <185, DBP <110 before bolus or procedure. |
| Post-IVT | SBP 140-180 × ≥24 h. Intensive <140 = no benefit (Class 3). |
| Post-EVT | <180/105 × 24 h. Intensive SBP <140 × 72 h after successful LVO recanalization = HARM (Class 3). |
LKW last known wellNIHSS NIH stroke scaleLVO large vessel occlusionIVT IV thrombolysisEVT endovascular thrombectomy
Acute Management
First moves. First hours.
Thrombolysis (within 4.5 h of LKW)
| Tenecteplase | 0.25 mg/kg IV bolus over 5-10 s (max 25 mg). Class 1, 2026. |
|---|---|
| Alteplase | 0.9 mg/kg (10% bolus, 90% over 60 min; max 90 mg). |
| LVO ≤4.5 h | TNK preferred over alteplase (2026, strong rec). |
Extended-window IVT (2026)
| 4.5-9 h or wake-up (2a) | If perfusion / DWI-FLAIR mismatch shows salvageable tissue. |
|---|---|
| 4.5-24 h LVO no EVT (2b) | Reasonable with imaging selection. |
Endovascular thrombectomy
| Standard window | LVO 0-6 h from LKW. |
|---|---|
| Extended window | 6-24 h with DAWN or DEFUSE-3 imaging selection. |
| IVT-eligible LVO | Give both IVT and EVT. Do not wait for one before the other. |
LKW last known wellIVT IV thrombolysisEVT endovascular thrombectomyLVO large vessel occlusionTNK tenecteplase
Pitfalls & Disposition
What gets missed.
What NOT to do (2026)
- Don't lower SBP <140 post-IVT or EVT. No benefit, possible harm.
- Don't pursue intensive glucose 80-130. Drives hypoglycemia.
- Don't give ASA as adjunct during alteplase infusion (Class 3).
- Don't delay IVT for INR or PTT if no known anticoagulation.
Secondary prevention
| AF screen | Telemetry, then 30-d ambulatory monitor. |
|---|---|
| Imaging | TTE (TEE if cryptogenic and <60). Carotid imaging. |
| Labs | Lipids, HbA1c. |
| Long-term Rx | High-intensity statin. BP <130/80. |
Posterior circulation strokes are commonly missed. Vertigo, nystagmus, ataxia, or diplopia: think basilar; get CTA.
IVT IV thrombolysisEVT endovascular thrombectomyASA aspirinTTE transthoracic echoTEE transesophageal echo
Sources
Verify against current guidelines and local protocol before acting.
- 2026 AHA/ASA Guidelines for Management of Acute Ischemic Stroke.
- AcT, NOR-TEST 2, TIMELESS: tenecteplase trials.
- DAWN (NEJM 2018), DEFUSE-3 (NEJM 2018): extended-window EVT.
Downloads
Every card for this topic — carousels and tables, print-ready for the wards or for sharing.