Sepsis & septic shock.
Sepsis-3 screening pitfalls, individualized fluid resuscitation (the 30 mL/kg mandate is gone), vasopressor ladder, source control as the intervention, and the 1-hour antibiotic gate.
Reviewed June 2026 · verify against current guidelines
Recognize. Confirm. Stage.
Sepsis-3 definitions
| Sepsis | Life-threatening organ dysfunction from dysregulated infection response. SOFA ↑ ≥2. |
|---|---|
| Septic shock | Sepsis + pressors for MAP ≥65 AND lactate >2 despite adequate fluids. |
Screening
qSOFA has low sensitivity — use as prompt, not gate. NEWS / institutional screens often outperform qSOFA.
Workup
Lactate, blood cx ×2 pre-abx, CBC/BMP/LFTs/coags, UA + urine cx, CXR, source imaging. Procalcitonin not for initiating abx; supports de-escalation.
First moves. First hours.
Antimicrobials
Empiric broad-spectrum targeting suspected source within 1 h for shock/probable sepsis. Cover MRSA, Pseudomonas per risk. De-escalate at 48-72 h.
Fluids (2026 SSC)
Balanced crystalloid > saline. ~30 mL/kg over 3 h but individualized — rigid mandate is gone. Reassess dynamically (PLR, US, IVC, refill). Avoid HES; albumin for large volumes.
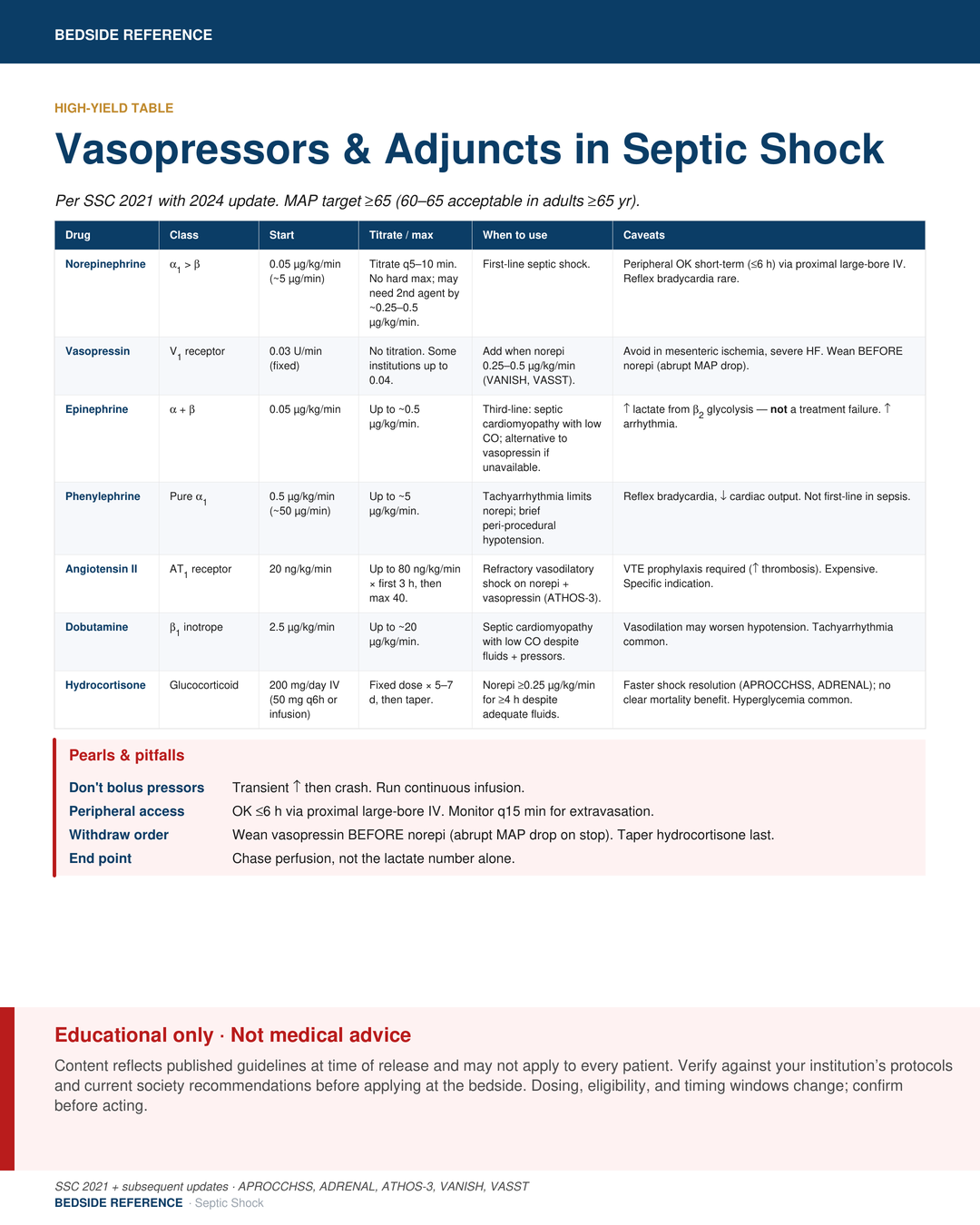
Vasopressors
Target MAP ≥65 (60-65 if ≥65 yr per 2026). 1st: norepi. Add: vasopressin 0.03 U/min. Refractory: epi; consider angiotensin II. Peripheral OK short-term. Hydrocortisone 200 mg/day if pressor-dependent.
What gets missed.
Reassess & adjuncts
Serial lactate clearance (q2–4 h until normal); capillary refill as adjunct. Chase perfusion, not a lactate number. Hydrocortisone if ongoing pressor need.
Source control
Drain, debride, decompress as early as feasible. Cholangitis, abscess, necrotizing infection, infected line, obstructive pyelo: source control IS the intervention.
Pitfalls
- Lactate ↑ has many causes (metformin, seizure, liver failure).
- 30 mL/kg in HF / ESRD / cirrhosis can harm.
- Delayed source control kills more than delayed antibiotics.
Sources
Verify against current guidelines and local protocol before acting.
- Surviving Sepsis Campaign: International Guidelines 2026. Crit Care Med / Intensive Care Med 2026.
- Singer M et al. Sepsis-3. JAMA 2016.
- ANDROMEDA-SHOCK; CLOVERS; CLASSIC trials informing 2026 fluid recommendations.
Downloads
Every card for this topic — carousels and tables, print-ready for the wards or for sharing.