Hypoglycemia.
Treat fast. Recheck. Find the cause. Definitions, the bedside fork (airway → access), pharm vs non-pharm etiologies, recurrent hypoglycemia workup, and discharge planning.
Reviewed June 2026 · verify against current guidelines
Classify. Find the cause.
Symptom, not a diagnosis
Find the cause before the next dose. Untreated etiology means recurrent events. Adjust the regimen before discharge.
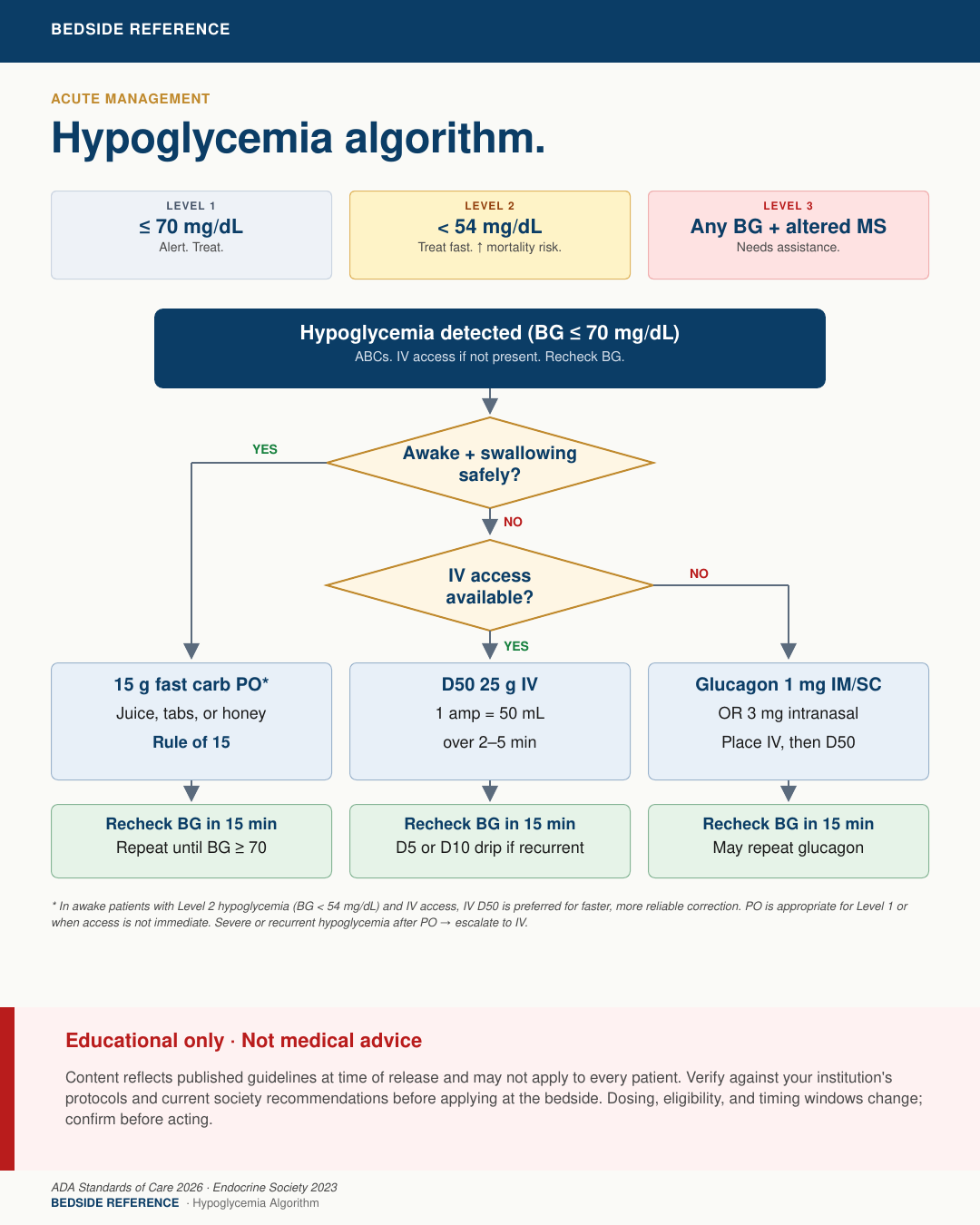
ADA classification (2026)
| Level 1 | BG 54–69 mg/dL (≤70 = alert value). Fast carb; hold or adjust glucose-lowering med. |
|---|---|
| Level 2 | BG <54 mg/dL. Treat now. Neuroglycopenia; higher mortality risk. |
| Level 3 | Any BG with altered status requiring assistance. IV or IM/IN glucagon. |
Treat by scenario.
First-line by scenario
| Awake, swallowing safely | 15 g fast carb PO (4 oz juice, 3–4 glucose tabs). Rule of 15: recheck 15 min, repeat to BG ≥70, then complex-carb meal. |
|---|---|
| NPO or BG <54, IV access | D50 25 g IV (1 amp = 50 mL) over 2–5 min. D10 200 mL (20 g) is an alternative with less rebound. Recheck 15 min. |
| Altered / unresponsive, no IV | Glucagon 1 mg IM/SC or 3 mg intranasal. Place IV ASAP, then D50. Fails if glycogen depleted. |
| Sulfonylurea-induced (any severity) | D50 PRN + octreotide 50–100 mcg SC q8h. Admit: effect outlasts dextrose. Recheck q1–2h × 12–24h. |
Refractory hypoglycemia.
Dextrose alone fails or hypoglycemia recurs. Usually long-acting insulin or sulfonylurea overdose, or adrenal insufficiency. ICU care; call endocrine, toxicology, and poison control.
Long-acting insulin overdose
| Infusion | D10W 100–200 mL/h. Titrate to BG 100–180. May need 7+ days after a massive overdose. |
|---|---|
| Monitor | BG q30–60 min, then q1–2h once stable. Continuous K+; check Na+ daily. |
| Octreotide | Consider 50–100 mcg SC q8h. Blunts dextrose-driven endogenous insulin. Thin, case-level evidence in insulin overdose. |
| Steroids | Stress-dose hydrocortisone (e.g. 100 mg IV q8h) as last-resort adjunct. Case-report evidence. |
What gets missed.
Don't miss
- Sulfonylurea hypoglycemia is admit-worthy. Discharge after one D50 amp will fail.
- Hypoglycemia in sepsis predicts mortality. Escalate; don't just feed glucose.
- Glucagon needs glycogen. Fails in alcohol use, malnutrition, fasting, or liver failure.
- Give thiamine before glucose in alcohol use or malnutrition.
- Recheck BG q15min until stable, then scheduled monitoring.
- Find and document the cause; adjust the regimen before discharge.
Prevent the next event.
Inpatient events recur. Fix the regimen before the next dose.
Inpatient adjustments (expert convention)
| NPO / poor PO | Hold prandial insulin. Reduce basal ~20–30%. Hold sulfonylureas. Keep correction scale. |
|---|---|
| AKI / renal | Clearance falls if eGFR <60. Reduce basal 25–50%. Stop sulfonylureas. Hold metformin. |
| Tube feeds off | Match basal to feeds. If feeds stop, start D10. |
| Steroid taper | Insulin requirement falls as steroids taper. Cut dose ~20%. Recheck BG TID. |
| After a hypo event | Reduce total daily dose ~20%. More if severe. |
Sources
Verify against current guidelines and local protocol before acting.
- ADA. Standards of Care in Diabetes 2026. Diabetes Care 2026;49(Suppl 1) (Level 1 = 54–69; Level 2 <54 mg/dL).
- McCall AL et al. Management of Individuals With Diabetes at High Risk for Hypoglycemia. Endocrine Society. J Clin Endocrinol Metab 2023;108(3):529–562.
- Cryer PE et al. Evaluation and Management of Adult Hypoglycemic Disorders. Endocrine Society Clinical Practice Guideline 2009.
- Fasano CJ et al. D10 vs D50 for ED hypoglycemia. Ann Emerg Med 2008 (less rebound, equivalent time to recovery).
- Glatstein M et al. Octreotide for sulfonylurea-induced hypoglycemia. Pediatr Emerg Care 2012.
- Demidowich AP et al. Prevention and Management of Insulin-Associated Hypoglycemia in Hospitalized Patients. Endocr Pract 2018 (≈20% TDD reduction after an event).
- FDA prescribing information: glucagon for injection (1 mg IM/SC/IV); intranasal glucagon (3 mg).
Downloads
Every card for this topic — carousels and tables, print-ready for the wards or for sharing.