DKA & HHS.
Updated ADA 2024 DKA criteria (β-OHB ≥3.0 is the new gate), HHS criteria, K-before-insulin fluid protocol, transition to SC insulin, euglycemic DKA triggers, and resolution by gap closure rather than glucose normalization.
Reviewed June 2026 · verify against current guidelines
Diagnosis & Workup
Recognize. Confirm. Stage.
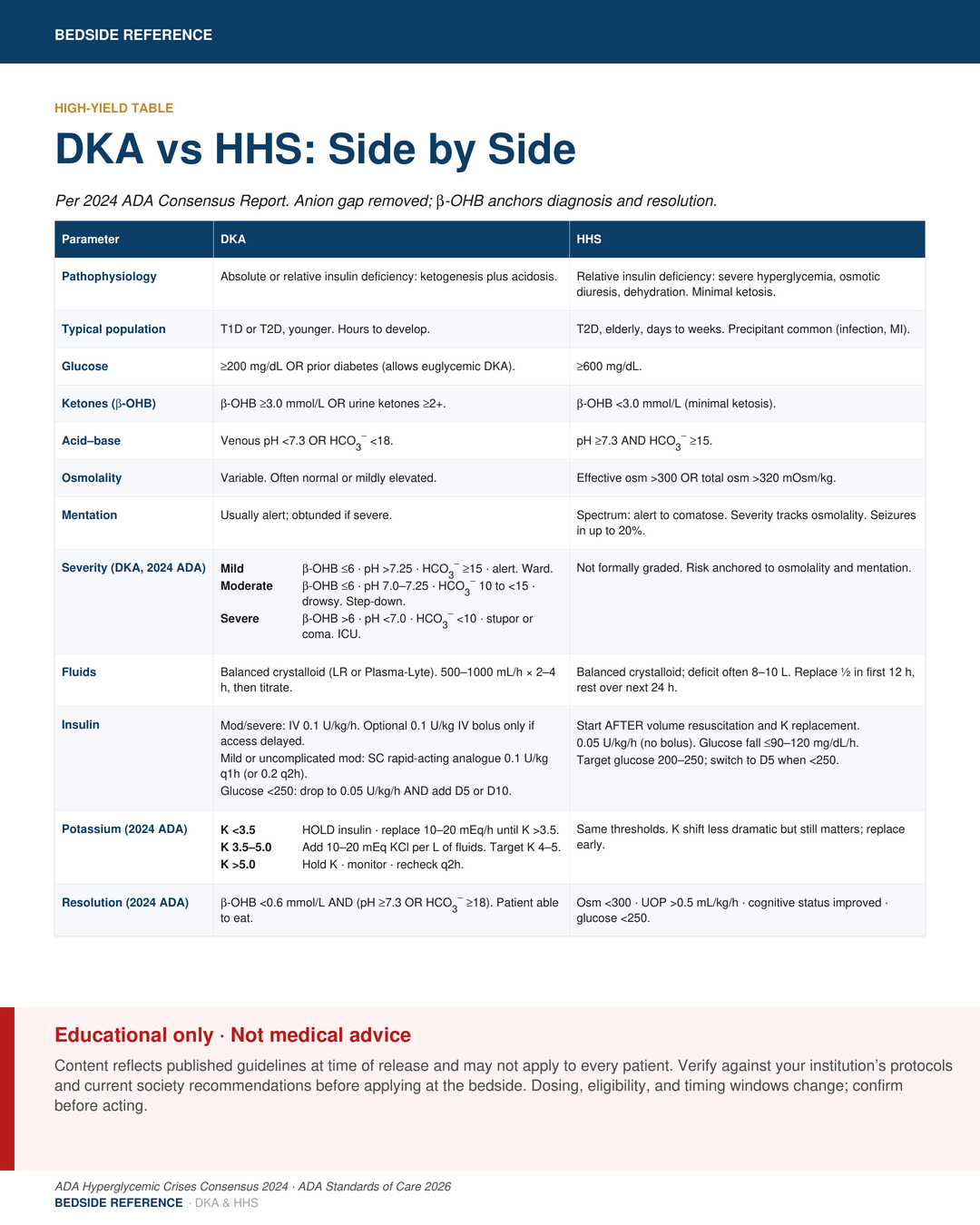
DKA criteria (2024 ADA, all 3)
| D | Glucose >200 mg/dL OR prior diabetes (allows euglycemic DKA) |
|---|---|
| K | β-hydroxybutyrate >3.0 mmol/L OR urine ketones ≥2+ |
| A | Venous pH <7.3 OR HCO3 |
DKA severity (2024 ADA)
| Mild | β-OHB <6 · pH >7.25 · HCO3 |
|---|---|
| Moderate | β-OHB <6 · pH 7.0-7.25 · HCO3 |
| Severe | β-OHB >6 · pH <7.0 · HCO3 |
HHS criteria (2024 ADA, all 4)
- Glucose >600 mg/dL
- Effective osm >300 OR total osm >320 mOsm/kg
- pH ≥7.3 AND HCO3
- ≥15 - β-OHB <3.0 mmol/L (or urine ketones <2+)
Euglycemic DKA: glucose can be <200. Triggers: SGLT2i, pregnancy, fasting or EtOH, prolonged vomiting in T1D.
HHS hyperosmolar hyperglycemic stateβ-OHB β-hydroxybutyrateSGLT2i SGLT2 inhibitorosm effective serum osmolality
Acute Management
Stabilization.
1) Fluids
| Choice | Balanced crystalloid (LR or Plasma-Lyte). |
|---|---|
| First 2-4 h | 500-1000 mL/h. |
| Then | 250-500 mL/h titrated to corrected Na and hemodynamics. |
| Older / HF / CKD | Smaller boluses (~250 mL) to avoid overload. |
2) Potassium (2024 ADA, check BEFORE insulin)
| K <3.5 | HOLD insulin · replace 10-20 mEq/h until K >3.5 |
|---|---|
| K 3.5-5.0 | Add 10-20 mEq KCl per L of fluids; target K 4-5 |
| K ≥5.0 | Hold K · monitor · recheck q2h |
LR lactated Ringer'sK potassiumKCl potassium chloride
Acute Management
Definitive therapy.
3) Insulin
| Mod / severe | Fixed-rate IV 0.1 U/kg/h. |
|---|---|
| IV bolus | 0.1 U/kg only if IV access is delayed. |
| Glucose <250 | Drop to 0.05 U/kg/h AND add D5 or D10. |
| Mild/uncomp mod | SC rapid-acting 0.1 U/kg q1h (or 0.2 U/kg q2h). |
4) Bicarbonate
| Indication | Reserved for pH <7.0 with hemodynamic instability. |
|---|---|
| Caveats | Rarely beneficial. Can worsen hypoK and cerebral edema. |
Monitoring
| Glucose | q1h while on drip. |
|---|---|
| Electrolytes / β-OHB / venous pH | q2–4 h until DKA resolved. |
| Mental status, UOP, vitals | Continuous; reassess fluid plan. |
SC subcutaneousD5/D10 5% / 10% dextroseβ-OHB β-hydroxybutyrate
Pitfalls & Disposition
Resolution & transition.
Resolution criteria (2024 ADA)
| DKA | β-OHB <0.6 mmol/L AND (pH ≥7.3 OR HCO3 |
|---|---|
| HHS | Osm <300 · UOP >0.5 mL/kg/h · cognitive status improved · glucose <250 |
Transition to SC insulin
| Timing | Start SC basal 1-2 h BEFORE stopping the drip (otherwise rebound DKA). |
|---|---|
| TDD | Insulin-naive: 0.3-0.6 U/kg/day basal/bolus. Otherwise resume home regimen. |
Disposition by severity
| Mild | Ward or observation unit. Standard nursing. |
|---|---|
| Moderate | Step-down or intermediate care. Closer monitoring. |
| Severe / HHS | ICU. Hourly checks, vasopressors if needed. |
β-OHB β-hydroxybutyrateUOP urine outputTDD total daily insulin doseHHS hyperosmolar hyperglycemic state
Pitfalls & Disposition
What gets missed.
HHS correction caps
| Glucose | Fall <90–120 mg/dL/h |
|---|---|
| Na | Fall <10 mmol/L per 24 h |
| Osm | Fall 3-8 mOsm/kg/h |
Pitfalls
- Following glucose alone. β-OHB or anion gap defines resolution.
- Stopping insulin when glucose normalizes drives recurrence.
- Missing the precipitant: infection, MI, missed insulin, drugs.
When to call
| ICU | Severe DKA (β-OHB >6, pH <7.0). HHS. AMS or coma. Hemodynamic instability. Cerebral edema. |
|---|---|
| Endocrine | Recurrent DKA. Refractory hyperglycemia. SGLT2i-DKA. Pregnancy. Complex insulin transition. |
SGLT2i with symptoms: check β-OHB even if glucose normal. Hold SGLT2i pre-op and in acute illness.
HHS hyperosmolar hyperglycemic stateβ-OHB β-hydroxybutyrateSGLT2i SGLT2 inhibitorMI myocardial infarction
Sources
Verify against current guidelines and local protocol before acting.
- ADA Hyperglycemic Crises in Adults: consensus report. Diabetes Care 2024.
- ADA Standards of Care 2026, Section 6 (glycemic goals, hypoglycemia, hyperglycemic crises).
- PLUS, SMART, SALT-ED: balanced crystalloid vs saline.
Downloads
Every card for this topic — carousels and tables, print-ready for the wards or for sharing.