Acute COPD exacerbation.
AECOPD definition and mimics, oxygen target 88–92% (hyperoxia kills), bronchodilator + 5-day prednisone per REDUCE, antibiotic criteria, NIV indications, and a discharge bundle where the most preventable readmission factor is inhaler technique.
Reviewed June 2026 · verify against current guidelines
Recognize. Confirm. Stage.
Definition (GOLD 2026)
Acute worsening of respiratory symptoms (↑ dyspnea, cough, sputum volume or purulence) requiring additional therapy.
Severity (Rome 2026, GOLD-adopted)
| Mild | Dyspnea VAS <5 · RR <24 · HR <95 · SpO2 ≥92% · CRP <10 |
|---|---|
| Moderate | Any of: VAS ≥5, RR ≥24, HR ≥95, SpO2 <92% or drop >3%, CRP ≥10 |
| Severe | Hypercapnia (PaCO2 >45) and/or acidosis (pH <7.35) |
Rule out mimics
| Differential | Pneumonia, acute HF or pulmonary edema, PE, pneumothorax, ACS, arrhythmia. |
|---|---|
| Workup | CXR, ECG, BNP, troponin. D-dimer if PE risk. |
First moves. First hours.
Treatment bundle
| Oxygen | Target SpO2 88-92%. Venturi mask to titrate. Recheck ABG 30-60 min. |
|---|---|
| Bronchodilators | SABA plus SAMA nebs (albuterol 2.5 mg, ipratropium 0.5 mg) q1–4 h, then q4–6 h. |
| Steroids | Prednisone 40 mg PO × 5 d (REDUCE). IV methylprednisolone if NPO or severe. |
| Antibiotics | Per GOLD 2026 criteria below. Duration 5 d. |
Antibiotic indications (GOLD 2026, any of)
| ≥2 cardinal sx | ↑ dyspnea, ↑ sputum volume, ↑ purulence. Purulence MUST be one. |
|---|---|
| Prior + culture | Positive sputum culture during a previous exacerbation. |
| On ventilation | Mechanical ventilation (invasive or NIV). |
Agent choice
| First-line | Amox/clav, doxycycline, or macrolide × 5 d. |
|---|---|
| Pseudomonas risk | Antipseudomonal β-lactam (e.g. pip-tazo, cefepime). |
What gets missed.
NIV (when and when not)
| Indications | Hypercapnic acidosis (pH <7.35, PaCO2 >45) · severe dyspnea with WOB · persistent hypoxemia |
|---|---|
| Contraindications | Respiratory arrest · hemodynamic instability · AMS · vomiting · copious secretions · facial trauma |
Intubation triggers
- NIV failure · arrest · refractory instability.
- Worsening AMS · persistent acidosis · cannot clear secretions.
Discharge bundle
- Inhaler technique verified. Watch them use it.
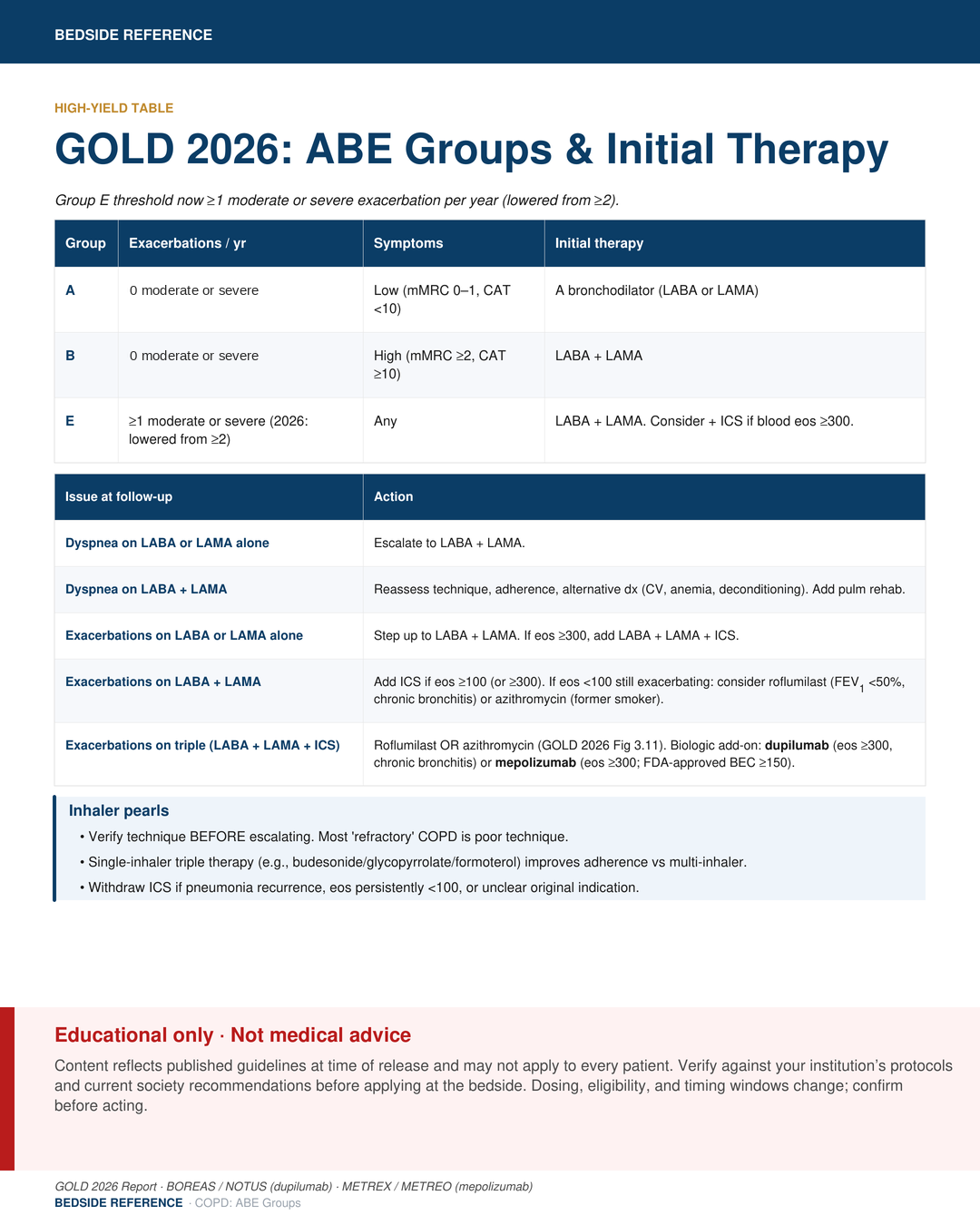
- Maintenance escalated if GOLD E (≥1 mod/severe per 2026).
- Pulm rehab referral, vaccines, smoking cessation, follow-up <4 weeks.
Sources
Verify against current guidelines and local protocol before acting.
- GOLD 2026 Global Strategy for Prevention, Diagnosis & Management of COPD.
- REDUCE trial (5-day vs 14-day prednisone). JAMA 2013.
- Anthonisen et al. Antibiotic use by cardinal symptoms in AECOPD. Ann Intern Med 1987.
- Brochard et al. Noninvasive ventilation in acute COPD exacerbation. NEJM 1995.
Downloads
Every card for this topic — carousels and tables, print-ready for the wards or for sharing.