Community-acquired pneumonia.
The 2025 ATS update: lung ultrasound as a CXR alternative, the pathogen/test map, CURB-65 + PSI and IDSA severity criteria, empiric coverage by setting, shorter courses (<5 days), and steroids in severe CAP — with the REMAP-CAP caveat against blind 7-day dosing.
Reviewed June 2026 · verify against current guidelines
Recognize. Confirm.
Clinical
Cough, fever, dyspnea, focal exam · new infiltrate on imaging.
Imaging
- CXR first.
- Lung ultrasound: acceptable alternative where expertise exists.
- CT if CXR negative and suspicion remains high.
Adjuncts
- Sputum + blood cultures: severe CAP, ICU, or MDR risk.
- Respiratory viral PCR: positive in healthy outpatient may obviate empiric abx.
- Procalcitonin does not exclude CAP. Do not withhold initial abx.
Know the bug.
Usual pathogens
| Typical | S. pneumoniae (#1) · H. influenzae · M. catarrhalis |
|---|---|
| Atypical | M. pneumoniae · C. pneumoniae · Legionella |
| Viral | Influenza · RSV · SARS-CoV-2. Co-infection common. |
| MDR | MRSA · Pseudomonas aeruginosa |
Targeted tests
| Urinary antigen | Pneumococcal: severe CAP. Legionella sg 1: severe, travel, outbreak. |
|---|---|
| Multiplex viral PCR | Flu · RSV · SARS-CoV-2 · others. Guides isolation + antivirals. |
| Flu + (severe / inpt) | Oseltamivir ASAP. Any duration from onset.* |
| Flu + (outpt) | Oseltamivir OR baloxavir within 48 h. |
| COVID + | Remdesivir OR nirmatrelvir-ritonavir per severity. |
*IV peramivir if oral / enteral oseltamivir not feasible.
Where they go.
CURB-65 (≥2 admit · ≥3 ICU)
| C | Confusion |
|---|---|
| U | BUN >19 mg/dL |
| R | RR ≥30 |
| B | SBP <90 / DBP ≤60 |
| 65 | Age ≥65 |
PSI (class → site)
| I-II | ≤70 pts → outpatient |
|---|---|
| III | 71–90 → obs / brief admit |
| IV | 91–130 → admit |
| V | >130 → ICU consider |
IDSA severe CAP criteria
Major (≥1) → ICU admission
| Respiratory failure requiring mechanical ventilation |
| Septic shock with need for vasopressors |
Minor (≥3) → severe CAP; consider ICU
| Respiratory | RR ≥30 · PaO2/FiO2 ≤250 · multilobar infiltrates |
|---|---|
| Neuro / metabolic | Confusion / disorientation · BUN ≥20 mg/dL |
| Hematologic | WBC <4,000* · platelets <100,000 |
| Other | Hypothermia <36°C · hypotension requiring aggressive fluid resuscitation |
*WBC <4,000 counts only if from infection alone (not chemotherapy or marrow suppression).
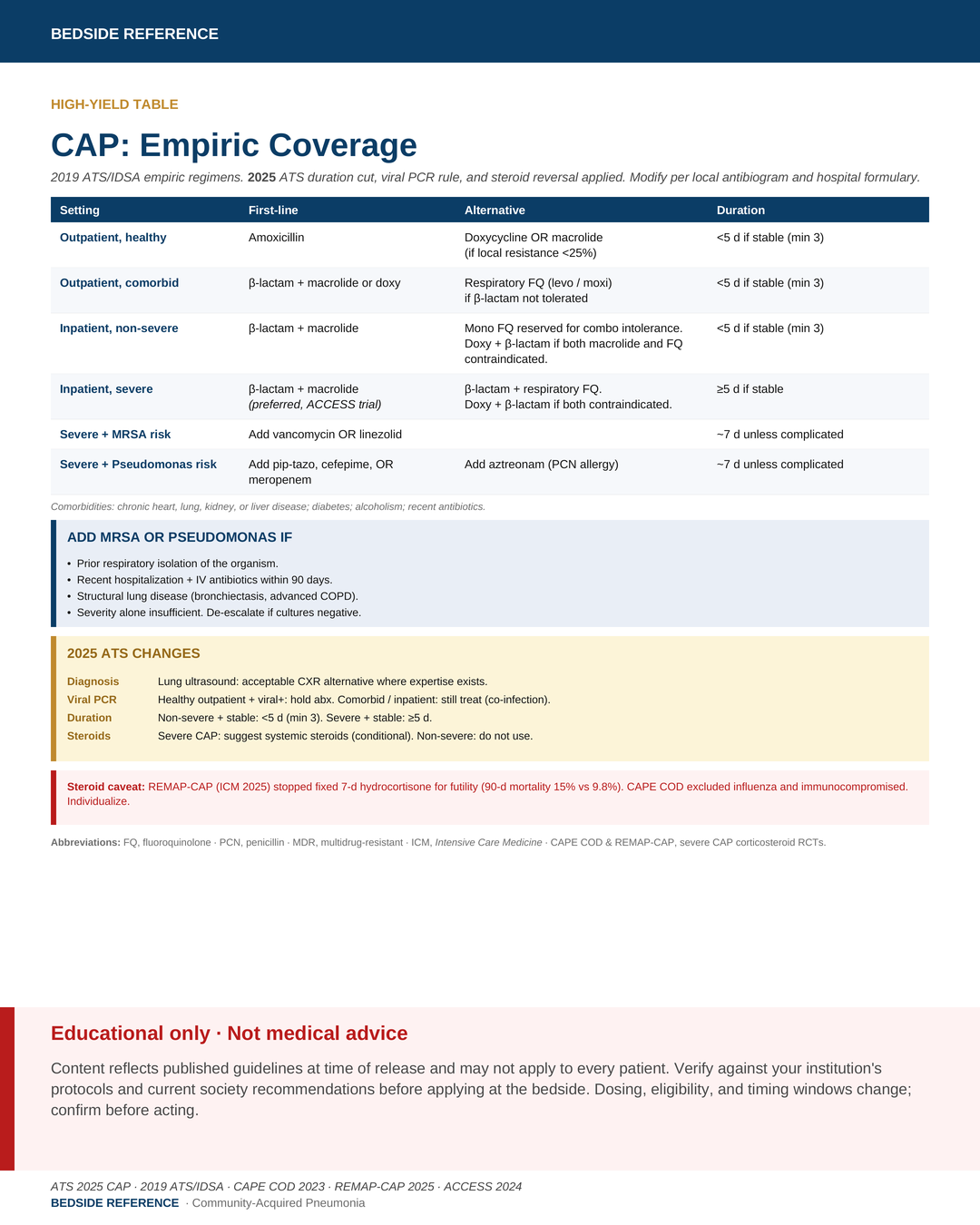
Empiric coverage.
Empiric regimens
| Outpatient, healthy | Amoxicillin OR doxycycline. Macrolide (if local resistance <25%). |
|---|---|
| Outpatient, comorbid | Combo: β-lactam + macrolide or doxy. Mono FQ (levo/moxi) if β-lactam not tolerated. |
| Inpatient, non-severe | Combo: β-lactam + macrolide. Mono FQ reserved for combo intolerance. Doxy if both macrolide and FQ contraindicated. |
| Inpatient, severe | β-lactam + macrolide preferred over FQ combo (ACCESS trial). Doxy if both contraindicated. |
Viral PCR positive
| Outpatient, no comorbidities | Hold antibiotics. |
|---|---|
| Outpatient with comorbidities | Still treat. |
| Any inpatient | Still treat. |
Comorbidities: chronic heart / lung / kidney / liver disease, diabetes, alcoholism, recent antibiotics.
β-lactams: (outpt) amox-clav, cefpodoxime, cefuroxime. (Inpt) ceftriaxone, cefotaxime, ampicillin-sulbactam.
Doxycycline preferred over macrolide (US pneumococcal resistance >30%).
What 2025 changed.
Duration: shorter if stable.
Steroids: 2019 don't; 2025 suggest in severe CAP.
Duration
| Outpatient + non-severe inpatient, stable | <5 days (min 3). |
|---|---|
| Severe CAP, stable | ≥5 days. |
| Stop when stable | VS normal · eating · baseline mentation. |
Steroids
| Non-severe CAP | Do not use. |
|---|---|
| Severe CAP | Suggest systemic steroids. |
| Excludes | Influenza · immunocompromised. |
REMAP-CAP (ICM 2025) stopped fixed 7-d hydrocortisone for futility: 90-d mortality 15% vs 9.8%. CAPE COD enrolled severe, non-influenza, non-immunosuppressed.
What gets missed.
Pitfalls
- Procalcitonin does not exclude CAP. Do not withhold initial abx.
- Holding abx in a comorbid patient because viral PCR is positive.
- Empiric MRSA / Pseudomonas coverage: requires risk factors, not severity alone.
- Steroids in influenza or immunocompromised CAP: CAPE COD excluded these groups.
Disposition
- Failure to improve by 72 h: reassess diagnosis, organism, drug.
- ATS/IDSA: routine follow-up imaging not recommended if symptoms resolve.
Sources
Verify against current guidelines and local protocol before acting.
- ATS. Diagnosis and Management of Community-Acquired Pneumonia. <i>AJRCCM</i> July 2025.
- Metlay JG et al. 2019 ATS/IDSA CAP guideline. <i>AJRCCM</i> 2019.
- Dequin PF et al. Hydrocortisone in Severe CAP (CAPE COD). <i>NEJM</i> 2023.
- REMAP-CAP Investigators. Hydrocortisone in Severe CAP. <i>ICM</i> 2025.
- Giamarellos-Bourboulis EJ et al. Clarithromycin in severe CAP (ACCESS). 2024.
Downloads
Every card for this topic — carousels and tables, print-ready for the wards or for sharing.