Acute kidney injury.
KDIGO criteria and staging, pre-renal vs intrinsic vs post-renal categorization, urine microscopy clues (muddy brown, WBC casts, RBC casts), drugs to hold or dose-adjust, and AEIOU indications for RRT.
Reviewed June 2026 · verify against current guidelines
Diagnosis & Workup
Recognize. Confirm. Stage.
KDIGO criteria (any of)
- SCr ↑ ≥0.3 mg/dL within 48 h
- SCr ↑ ≥1.5× baseline in 7 days
- Urine output <0.5 mL/kg/h × 6 h
Staging (KDIGO)
| Stage | SCr | Urine output |
|---|---|---|
| Stage 1 | 1.5-1.9× baseline OR ↑ ≥0.3 mg/dL | <0.5 mL/kg/h × 6-12 h |
| Stage 2 | 2.0-2.9× baseline | <0.5 mL/kg/h × ≥12 h |
| Stage 3 | ≥3× baseline OR SCr >4.0 OR RRT | <0.3 mL/kg/h × 24 h OR anuria ≥12 h |
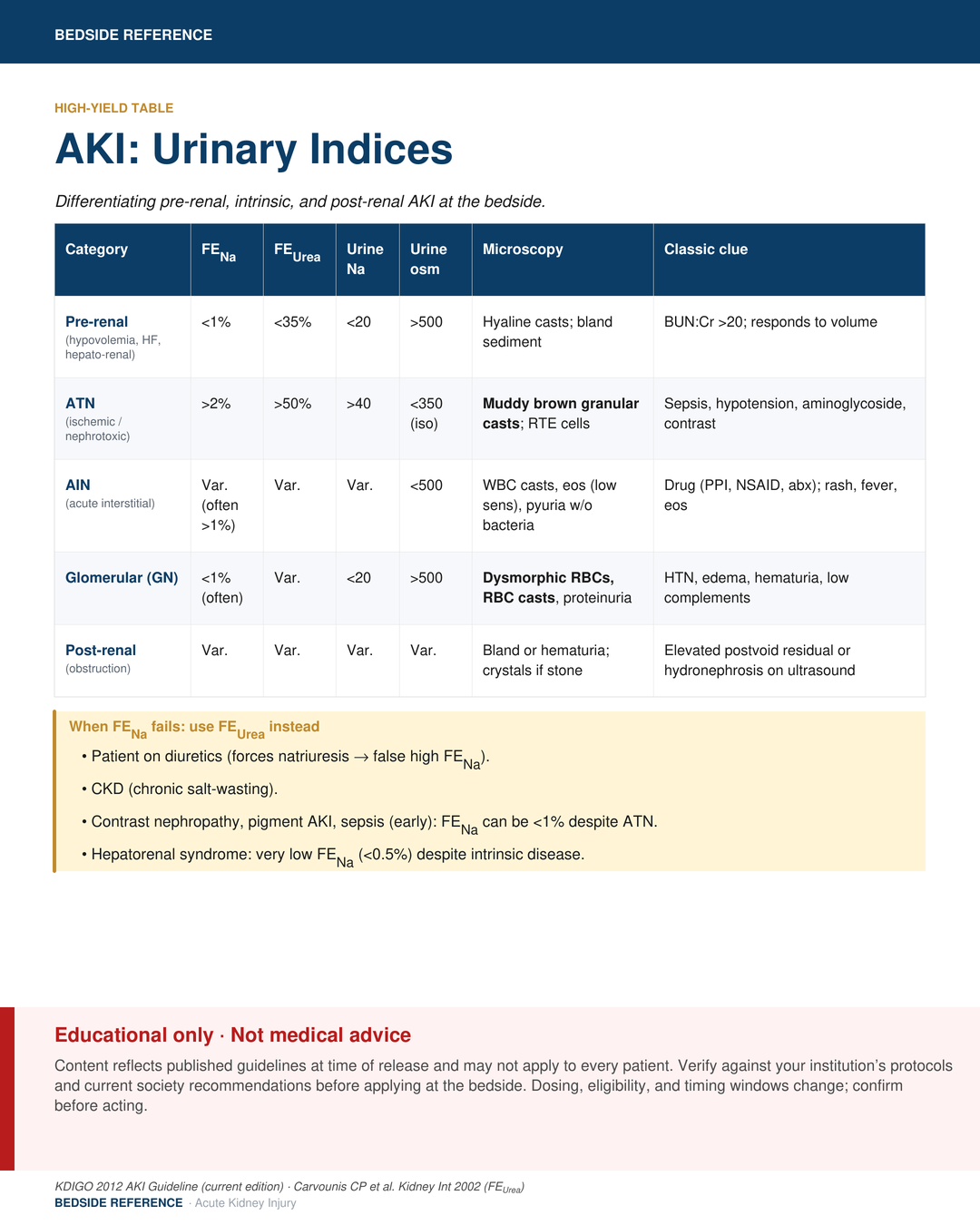
Categorize the cause
- Pre-renal: hypovolemia, HF, cirrhosis, NSAIDs, ACEi/ARB.
- Intrinsic: ATN (most common), AIN, GN, vascular, pigment.
- Post-renal: obstruction.
SCr serum creatinineUOP urine outputATN acute tubular necrosisAIN acute interstitial nephritisGN glomerulonephritis
Acute Management
First moves. First hours.
Three principles
- Restore perfusion: judicious fluids if pre-renal; balanced crystalloid.
- Treat the cause: relieve obstruction, treat sepsis, stop the offender.
- Avoid further injury: hold nephrotoxins, renally dose meds.
Drugs to hold / dose-adjust
| Hold | NSAIDs · ACEi/ARB (case-by-case in HF) · nephrotoxic abx · iodinated contrast |
|---|---|
| Dose-adjust | LMWH · DOACs · gabapentin · allopurinol · metformin (hold if Stage 2+) |
Urine microscopy clues
| Muddy brown casts | ATN |
|---|---|
| WBC casts / eos | AIN |
| RBC casts | GN |
| Bland sediment | Pre-renal or post-renal |
LMWH low-molecular-weight heparinDOAC direct oral anticoagulantATN acute tubular necrosisAIN acute interstitial nephritisGN glomerulonephritis
Pitfalls & Disposition
What gets missed.
RRT indications (AEIOU)
| A | Acidosis (severe, refractory) |
|---|---|
| E | Electrolytes (refractory hyperK) |
| I | Ingestions (toxic alcohols, lithium, salicylate) |
| O | Overload (refractory) |
| U | Uremia (pericarditis, encephalopathy, bleeding) |
Common pitfalls
- Reflexive fluids in HF or cirrhosis worsens AKI. Assess volume first.
- ACEi/ARB-induced Cr rise <30% is expected and acceptable.
- Contrast nephropathy is over-diagnosed; indicated contrast rarely withheld.
- HRS needs albumin plus vasoconstrictor, not aggressive crystalloid.
Refractory hyperK with ECG changes, severe acidosis, or uremic complications: call nephrology now.
RRT renal replacement therapyhyperK hyperkalemiaHRS hepatorenal syndrome
Sources
Verify against current guidelines and local protocol before acting.
- KDIGO 2012 Clinical Practice Guideline for AKI. Kidney Int Suppl. 2012;2:1–138 (still the published guideline).
- KDIGO 2026 AKI/AKD draft (public comment closed Apr 2026; final pending).
- STARRT-AKI trial (timing of RRT). NEJM 2020.
- BICAR-ICU (bicarbonate in severe acidemia). Lancet 2018.
Downloads
Every card for this topic — carousels and tables, print-ready for the wards or for sharing.