HFrEF — GDMT four pillars.
Starting and target doses for ARNI, β-blocker, MRA, SGLT2i — plus the 2024 ECDP add-ons (vericiguat, finerenone, IV iron). Order of initiation, K/Cr monitoring, and the STRONG-HF in-hospital case.
Reviewed June 2026 · verify against current guidelines
STRONG-HF: in-hospital initiation of all four GDMT pillars cut HF death + readmission by 34%. Start them before discharge.
The four pillars
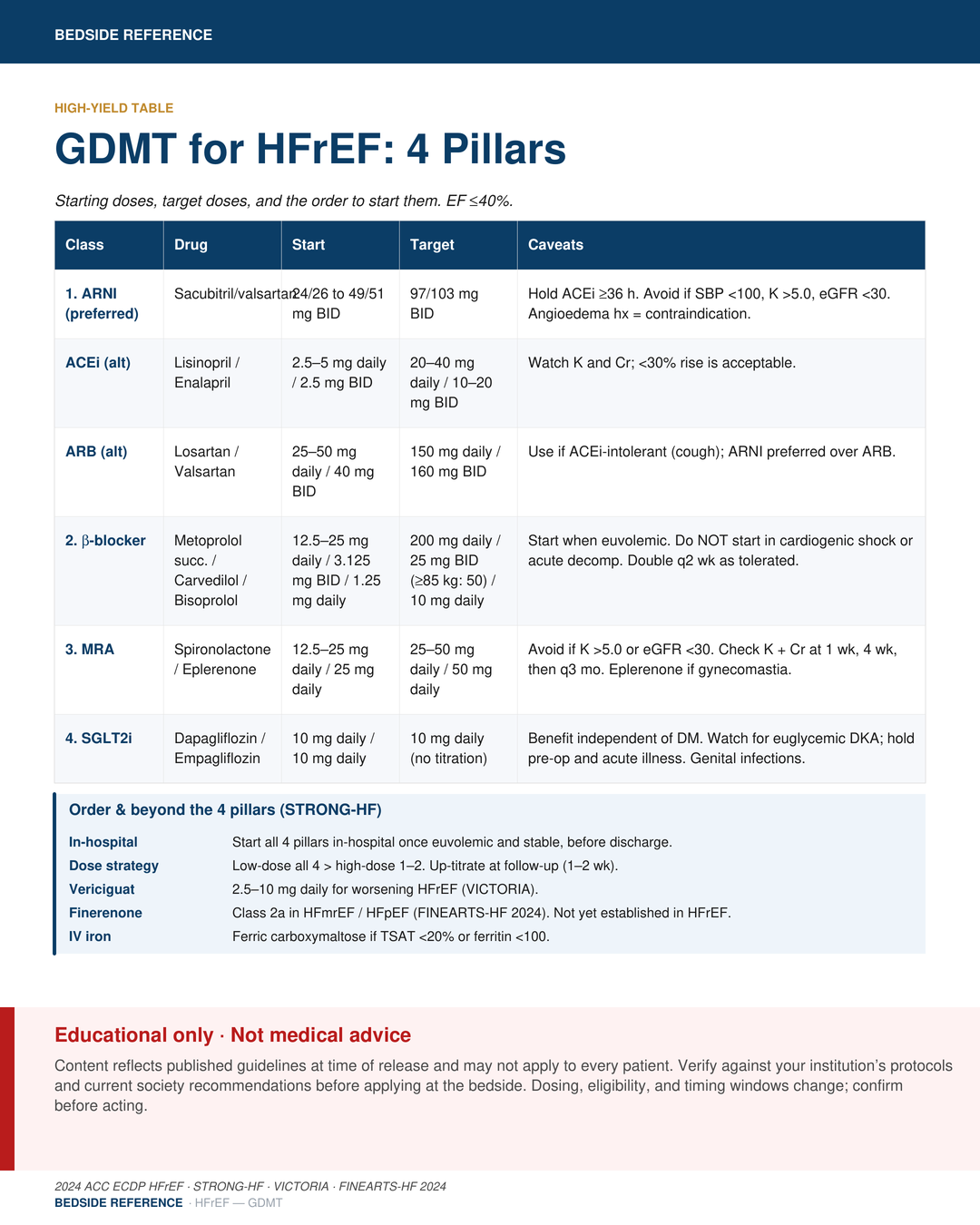
Start all four. EF ≤40%.
GDMT pillars — start & target doses
| Class | Drug | Start | Target | Caveats |
|---|---|---|---|---|
| 1. ARNI (preferred) | Sacubitril/valsartan | 24/26 to 49/51 mg BID | 97/103 mg BID | Hold ACEi ≥36 h before first dose. Avoid if SBP <100, K >5.0, eGFR <30. Angioedema history = contraindication. |
| ACEi (alt) | Lisinopril / enalapril | 2.5–5 mg daily / 2.5 mg BID | 20–40 mg daily / 10–20 mg BID | Watch K and Cr; a <30% rise in Cr is acceptable. |
| ARB (alt) | Losartan / valsartan | 25–50 mg daily / 40 mg BID | 150 mg daily / 160 mg BID | Use if ACEi-intolerant (cough); ARNI preferred over ARB. |
| 2. β-blocker | Metoprolol succinate / carvedilol / bisoprolol | 12.5–25 mg daily / 3.125 mg BID / 1.25 mg daily | 200 mg daily / 25 mg BID (≥85 kg: 50) / 10 mg daily | Start only when euvolemic. Do NOT start in cardiogenic shock or acute decompensation. Double every 2 wk as tolerated. |
| 3. MRA | Spironolactone / eplerenone | 12.5–25 mg daily / 25 mg daily | 25–50 mg daily / 50 mg daily | Avoid if K >5.0 or eGFR <30. Check K + Cr at 1 wk, 4 wk, then q3 mo. Eplerenone if gynecomastia. |
| 4. SGLT2i | Dapagliflozin / empagliflozin | 10 mg daily | 10 mg daily (no titration) | Benefit is independent of diabetes. Watch for euglycemic DKA; hold pre-op and in acute illness. Genital infections. |
Order & beyond
Sequencing and the add-ons.
Order & beyond the 4 pillars (STRONG-HF)
| In-hospital | Start all four pillars in-hospital once euvolemic and stable, before discharge. |
|---|---|
| Dose strategy | Low-dose all four → up-titrate 1–2 at a time. Reassess at follow-up (1–2 wk). |
| Vericiguat | 2.5–10 mg daily for worsening HFrEF (VICTORIA). |
| Finerenone | Class 2a in HFmrEF / HFpEF (FINEARTS-HF 2024). Not yet established in HFrEF. |
| IV iron | Ferric carboxymaltose if TSAT <20% or ferritin <100. |
ARNI angiotensin receptor–neprilysin inhibitorACEi angiotensin-converting enzyme inhibitorARB angiotensin receptor blockerMRA mineralocorticoid receptor antagonistSGLT2i sodium-glucose cotransporter-2 inhibitorEF ejection fractionSBP systolic blood pressureeGFR estimated glomerular filtration rateTSAT transferrin saturationHFrEF HF with reduced EF
Sources
Verify against current guidelines and local protocol before acting.
- 2022 AHA/ACC/HFSA Heart Failure Guideline
- 2024 ACC Expert Consensus Decision Pathway for HFrEF
- STRONG-HF
- VICTORIA
- FINEARTS-HF 2024
Downloads
Every card for this topic — carousels and tables, print-ready for the wards or for sharing.