Acute coronary syndrome.
ECG in 10 min. hs-troponin 0/1-2 h. PCI on the clock. STEMI vs NSTE-ACS pathways, the high-sensitivity troponin algorithm, antiplatelet + anticoagulation choices, and reperfusion windows.
Reviewed June 2026 · verify against current guidelines
Recognize. Confirm. Stage.
First 10 minutes
- ECG ≤10 min from FMC (incl. prehospital).
- Repeat ECG: recurrent sx · hemodynamic change · high suspicion.
- hs-cTn at 0 and 1-2 h (conventional cTn: 0 and 3-6 h).
STEMI ECG criteria
| Most leads | ST elevation ≥1 mm in ≥2 contiguous leads (outside V2-V3). |
|---|---|
| V2-V3 | ≥2 mm men ≥40 y · ≥2.5 mm men <40 y · ≥1.5 mm women. |
| Posterior MI | ST depression ≥0.5 mm in V1-V3 → obtain V7-V9. STE ≥0.5 mm in V7-V9 confirms. |
| LBBB or paced | NOT a STEMI equivalent in isolation. Requires clinical correlation. |
NSTE-ACS ECG (any of; normal does NOT exclude)
| ST depression | ≥0.5 mm in ≥2 contig leads, horizontal/downsloping · new or dynamic. |
|---|---|
| T-wave inversion | >1 mm in ≥2 contig leads with dominant R. |
| Transient STE | Self-resolving ST elevation. |
NSTE-ACS = symptoms without persistent STE; ↑ troponin (NSTEMI).
UA = symptoms + non-diagnostic ECG + normal troponin (historical category; now largely reclassified as NSTE-ACS in the hs-cTn era).
OMI patterns to know.
Standard ED teaching, not in the 2025 ACS guideline. Useful when ECG looks "not quite STEMI" but artery is occluded.
Patterns
| Posterior MI | STD ≥0.5 mm in V1-V3 + tall R waves → V7-V9 (STE ≥0.5 mm confirms). |
|---|---|
| deWinter T | Upsloping STD at J point + tall symmetric T waves V1-V6 → proximal LAD. |
| Wellens | Biphasic (Type A) or deeply inverted (Type B) T in V2-V3 during pain-free interval → critical LAD; AVOID stress. |
| aVR + diffuse STD | STE aVR + diffuse STD → LMCA, proximal LAD, or 3-vessel disease. |
Sgarbossa criteria (LBBB or paced rhythm)
| Concordant STE | ≥1 mm in any lead with positive QRS (highly specific). |
|---|---|
| Concordant STD | ≥1 mm in V1, V2, or V3 (highly specific). |
| Discordant STE | Original: ≥5 mm with negative QRS. Modified (Smith): ST/S ratio ≥ 0.25 (more sensitive). |
Antiplatelet + anticoagulation.
DAPT
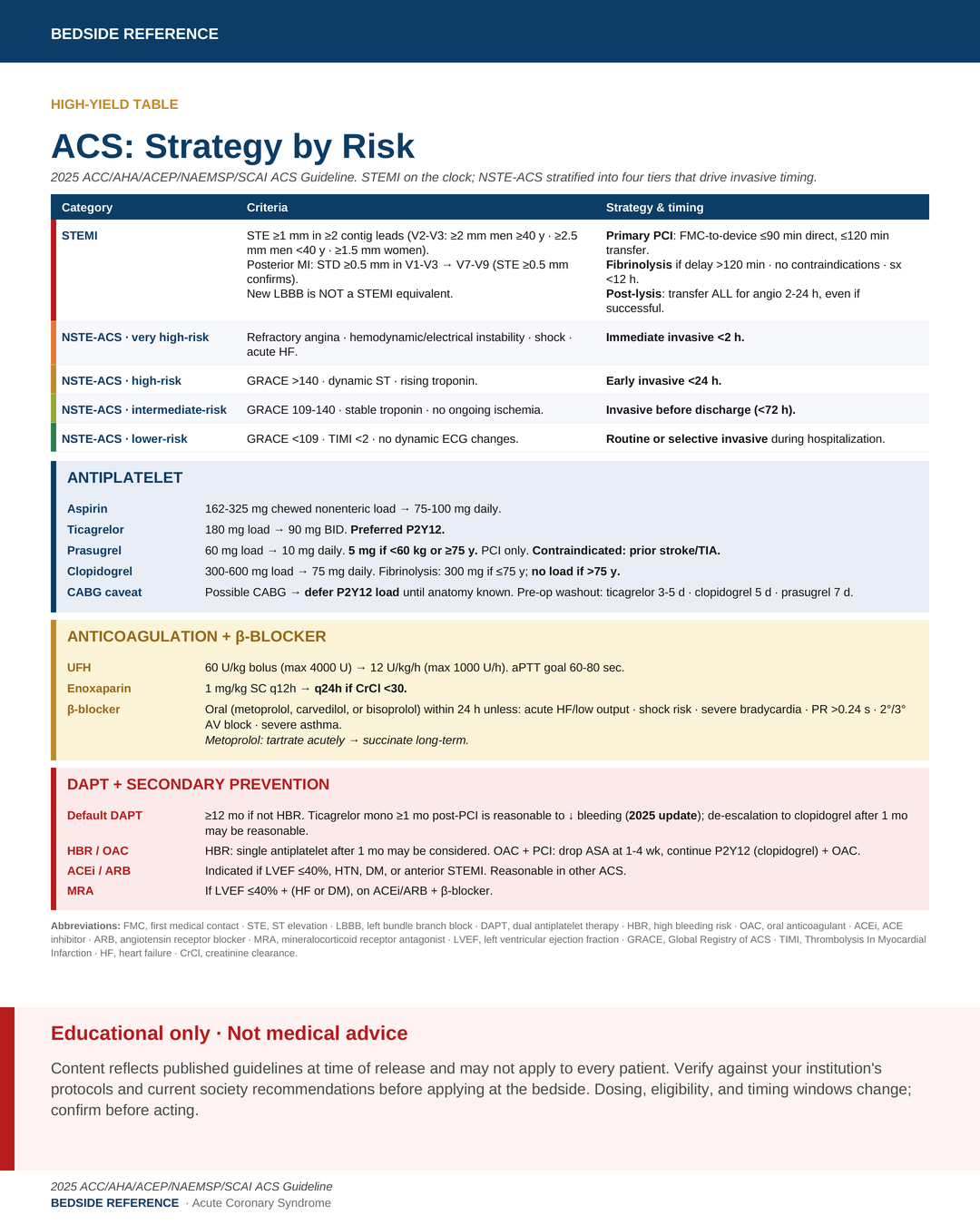
| Aspirin | 162-325 mg chewed nonenteric load → 75-100 mg daily. |
|---|---|
| Ticagrelor | 180 mg load → 90 mg BID. Preferred P2Y12. |
| Prasugrel | 60 mg load → 10 mg daily. 5 mg if <60 kg or ≥75 y. PCI only. |
| Clopidogrel | 300-600 mg load → 75 mg daily. Fibrinolysis: 300 mg if ≤75 y; no load if >75 y. |
Anticoagulation
| UFH | 60 U/kg bolus (max 4000 U) → 12 U/kg/h (max 1000 U/h). aPTT goal 60-80 sec. |
|---|---|
| Enoxaparin | 1 mg/kg SC q12h → q24h if CrCl <30. |
β-blocker
| Within 24 h | Oral β-blocker (metoprolol, carvedilol, or bisoprolol) unless: acute HF/low output · shock risk · severe bradycardia · PR >0.24 s · 2°/3° AV block · severe asthma. Metoprolol: tartrate acutely → succinate long-term. |
|---|
In NSTE-ACS without an invasive plan, ticagrelor is preferred over prasugrel.
If CABG is possible, defer the P2Y12 load until coronary anatomy is known (pre-op washout: ticagrelor 3-5 d · clopidogrel 5 d · prasugrel 7 d).
On the clock.
STEMI timing
| PCI direct | FMC-to-device ≤90 min. |
|---|---|
| PCI transfer | FMC-to-device ≤120 min. |
| Fibrinolysis | Anticipated PCI delay >120 min · no contraindications · sx <12 h. |
| Post-lysis | Transfer ALL for angio 2-24 h, even if successful. |
NSTE-ACS invasive timing
| Immediate <2 h | Very high-risk: refractory angina · hemodynamic/electrical instability · shock · acute HF. |
|---|---|
| Early <24 h | High-risk: GRACE >140 · dynamic ST · rising troponin. |
| <72 h before d/c | Intermediate-risk: GRACE 109-140 · stable troponin · no ongoing ischemia. |
| Routine or selective | Lower-risk: GRACE <109 · TIMI <2. |
Procedural standards
| Access | Radial > femoral. |
|---|---|
| Imaging | IVUS or OCT for complex PCI. |
| Complete revasc | Stable STEMI + MVD → revasc non-IRA. Shock → culprit-only. |
What gets missed.
Common errors
- Supplemental O2 when SpO2 ≥90% — no benefit, possible harm.
- Prasugrel after prior stroke or TIA — contraindicated.
- Loading P2Y12 pre-cath when CABG possible → delays urgent surgery.
- Skipping CrCl before enoxaparin or contrast.
- Calling new LBBB a STEMI equivalent.
- Treating posterior or deWinter pattern as "just ST depression."
- Forgetting post-lysis transfer for 2-24 h angio.
Transfusion (MINT)
| Threshold | Hb ~10 g/dL reasonable in ACS + acute/chronic anemia, no active bleeding. |
|---|
DAPT strategy + discharge.
DAPT duration & de-escalation
| Default | DAPT ≥12 mo if not HBR. |
|---|---|
| Ticagrelor mono | DAPT → ticagrelor alone ≥1 mo post-PCI is reasonable to ↓ bleeding. |
| De-escalate | Ticagrelor or prasugrel → clopidogrel after 1 mo may be reasonable to ↓ bleeding. |
| HBR | Single antiplatelet after 1 mo may be considered. |
| OAC + PCI | Drop aspirin at 1-4 wk; continue P2Y12 (clopidogrel preferred) + OAC. |
Secondary prevention
| Statin | High-intensity. Add ezetimibe if LDL-C ≥70 on max statin. |
|---|---|
| ACEi / ARB | Indicated if LVEF ≤40%, HTN, DM, or anterior STEMI. Reasonable in other ACS. |
| MRA | If LVEF ≤40% with HF or DM, on ACEi/ARB + β-blocker. |
| Cardiac rehab | Refer all. Home-based acceptable. |
Sources
Verify against current guidelines and local protocol before acting.
- Rao SV et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes. Circulation 2025;151:e771-e862 (copublished JACC 2025;85:2135-2237).
- Thiele H et al. CULPRIT-SHOCK: culprit-only vs multivessel PCI in cardiogenic shock. NEJM 2017.
- Carson JL et al. MINT: restrictive vs liberal transfusion in MI + anemia. NEJM 2023.
- Mehran R et al. TWILIGHT: ticagrelor monotherapy after PCI. NEJM 2019.
Downloads
Every card for this topic — carousels and tables, print-ready for the wards or for sharing.